Chapter 10: Lifespan Development
10.4 Development in Adolescence and Adulthood
Learning Objectives
- Describe physical, cognitive, and emotional development that occurs during adolescence
- Describe physical, cognitive, and emotional development that occurs in adulthood
- Differentiate between fluid and crystallized intelligence
- Explain attitudes toward death and Kübler-Ross’s five stages of grief (denial, anger, bargaining, depression, acceptance)
Introduction to Development in Adolescence and Adulthood
Changes in development during childhood are rapid and more obvious than the changes that come later on in life, but before you reach adulthood, there is one more large transition: adolescence. Adolescence brings the physical development of puberty, as well as cognitive, social, and emotional changes. Following adolescence, transitions are less obvious, but still significant throughout emerging adulthood and adulthood. Finally, growing older means confronting many psychological, emotional, and social issues that come with entering the last phase of life.
Watch It
Watch this video from a few of the world’s oldest people for some advice on how you can also live a fulfilling life until the very end.
You can view the transcript for “How to Be the Oldest Person Alive” here (opens in new window).
Adolescence
Adolescence is a socially constructed concept. In pre-industrial society, children were considered adults when they reached physical maturity, but today we have an extended time between childhood and adulthood called adolescence. Adolescence is the period of development that begins at puberty and ends at emerging adulthood, or into the mid- to late 20s. In the United States, adolescence is seen as a time to develop independence from parents while remaining connected to them (Figure 1). The typical age range of adolescence is from 12 to 18 years, and this stage of development also has some predictable physical, cognitive, and psychosocial milestones.

Physical Development
As noted above, adolescence begins with puberty. While the sequence of physical changes in puberty is predictable, the onset and pace of puberty vary widely. Several physical changes occur during puberty, such as adrenarche and gonadarche, the maturing of the adrenal glands and sex glands, respectively. Also during this time, primary and secondary sexual characteristics develop and mature. Primary sexual characteristics are organs specifically needed for reproduction, like the uterus and ovaries in females and testes in males. Secondary sexual characteristics are physical signs of sexual maturation that do not directly involve sex organs, such as development of breasts and hips in girls, and development of facial hair and a deepened voice in boys. Girls experience menarche, the beginning of menstrual periods, usually around 12–13 years old, and boys experience spermarche, the first ejaculation, around 13–14 years old.
During puberty, both sexes experience a rapid increase in height (i.e., growth spurt). For girls this begins between 8 and 13 years old, with adult height reached between 10 and 16 years old. Boys begin their growth spurt slightly later, usually between 10 and 16 years old, and reach their adult height between 13 and 17 years old. Both nature (i.e., genes) and nurture (e.g., nutrition, medications, and medical conditions) can influence height.
Because rates of physical development vary so widely among teenagers, puberty can be a source of pride or embarrassment. Early maturing boys tend to be stronger, taller, and more athletic than their later maturing peers. They are usually more popular, confident, and independent, but they are also at a greater risk for substance abuse and early sexual activity (Flannery, Rowe, & Gulley, 1993; Kaltiala-Heino, Rimpela, Rissanen, & Rantanen, 2001). Early maturing girls may be teased or overtly admired, which can cause them to feel self-conscious about their developing bodies. These girls are at a higher risk for depression, substance abuse, and eating disorders (Ge, Conger, & Elder, 2001; Graber, Lewinsohn, Seeley, & Brooks-Gunn, 1997; Striegel-Moore & Cachelin, 1999). Late blooming boys and girls (i.e., they develop more slowly than their peers) may feel self-conscious about their lack of physical development. Negative feelings are particularly a problem for late maturing boys, who are at a higher risk for depression and conflict with parents (Graber et al., 1997) and more likely to be bullied (Pollack & Shuster, 2000).
The adolescent brain also remains under development. Recall from your earlier study, that the brain consists of six regions: temporal lobe, brain stem, cerebellum, occipital lobe (includes the visual cortex), parietal lobe, and the frontal lobe. The frontal lobe consists of the prefrontal cortex, premotor cortex, and motor cortex. The prefrontal lobe lies just behind the forehead. Up until puberty, brain cells continue to bloom in the frontal region. Adolescents engage in increased risk-taking behaviors and emotional outbursts possibly because the frontal lobes of their brains are still developing (Figure 2). Recall that this area is often called the “CEO of the brain”, as it is responsible for judgment, impulse control, and planning. It is still maturing into early adulthood, up until around age 25 (Casey, Tottenham, Liston, & Durston, 2005).

Brain maturity occurs when there is growth of new neural connections and the pruning of unused neurons and connections. According to recent research, the brain regions tend to develop from the back to the front of the brain. Also, myelin continues to grow around axons and neurons helping to speed transmission between the various regions of the brain.
Cognitive Development

Psychosocial Development
Adolescents continue to refine their sense of self as they relate to others. Erikson referred to the task of the adolescent as one of identity versus role confusion. Thus, in Erikson’s view, an adolescent’s main questions are “Who am I?” and “Who do I want to be?” Some adolescents adopt the values and roles that their parents expect for them. Other teens develop identities that are in opposition to their parents but align with a peer group. This is common as peer relationships become a central focus in adolescents’ lives.
As adolescents work to form their identities, they pull away from their parents, and the peer group becomes very important (Shanahan, McHale, Osgood, & Crouter, 2007). Despite spending less time with their parents, most teens report positive feelings toward them (Moore, Guzman, Hair, Lippman, & Garrett, 2004). Warm and healthy parent-child relationships have been associated with positive child outcomes, such as better grades and fewer school behavior problems, in the United States as well as in other countries (Hair et al., 2005).
It appears that most teens don’t experience adolescent storm and stress to the degree once famously suggested by G. Stanley Hall, a pioneer in the study of adolescent development. Only small numbers of teens have major conflicts with their parents (Steinberg & Morris, 2001), and most disagreements are minor. For example, in a study of over 1,800 parents of adolescents from various cultural and ethnic groups, Barber (1994) found that conflicts occurred over day-to-day issues such as homework, money, curfews, clothing, chores, and friends. These types of arguments tend to decrease as teens develop (Galambos & Almeida, 1992).
Emerging Adulthood
The next stage of development is emerging adulthood. This is a relatively newly defined period of lifespan development spanning from 18 years old to the mid-20s, characterized as an in-between time where identity exploration is focused on work and love.
When does a person become an adult? There are many ways to answer this question. In the United States, you are legally considered an adult at 18 years old. But other definitions of adulthood vary widely; in sociology, for example, a person may be considered an adult when she becomes self-supporting, chooses a career, gets married, or starts a family. The ages at which we achieve these milestones vary from person to person as well as from culture to culture. For example, in the African country of Malawi, 15-year-old Njemile was married at 14 years old and had her first child at 15 years old. In her culture she is considered an adult. Children in Malawi take on adult responsibilities such as marriage and work (e.g., carrying water, tending babies, and working fields) as early as 10 years old. In stark contrast, independence in Western cultures is taking longer and longer, effectively delaying the onset of adult life.
Why is it taking twenty-somethings so long to grow up? It seems that emerging adulthood is a product of both Western culture and our current times (Arnett, 2000). People in developed countries are living longer, allowing the freedom to take an extra decade to start a career and family. Changes in the workforce also play a role. For example, 50 years ago, a young adult with a high school diploma could immediately enter the work force and climb the corporate ladder. That is no longer the case. Bachelor’s and even graduate degrees are required more and more often—even for entry-level jobs (Arnett, 2000). In addition, many students are taking longer (five or six years) to complete a college degree as a result of working and going to school at the same time. After graduation, many young adults return to the family home because they have difficulty finding a job. Changing cultural expectations may be the most important reason for the delay in entering adult roles. Young people are spending more time exploring their options, so they are delaying marriage and work as they change majors and jobs multiple times, putting them on a much later timetable than their parents (Arnett, 2000).
Link to Learning
Review these concepts on adolescence and emerging adulthood in the Crash Course Psychology video.
Think It Over
Would you describe your experience of puberty as one of pride or embarrassment? Why?
Adulthood
Adulthood begins around 20 years old and has three distinct stages: early, middle, and late. Each stage brings its own set of rewards and challenges.
Physical Development

By the time we reach early adulthood (20 to early 40s), our physical maturation is complete, although our height and weight may increase slightly. In young adulthood, our physical abilities are at their peak, including muscle strength, reaction time, sensory abilities, and cardiac functioning. Most professional athletes are at the top of their game during this stage. Many women have children in the young adulthood years, so they may see additional weight gain and breast changes.
Middle adulthood extends from the 40s to the 60s (Figure 1). Physical decline is gradual. The skin loses some elasticity, and wrinkles are among the first signs of aging. Visual acuity decreases during this time. Women experience a gradual decline in fertility as they approach the onset of menopause, the end of the menstrual cycle, around 50 years old. Both men and women tend to gain weight: in the abdominal area for men and in the hips and thighs for women. Hair begins to thin and turn gray.
Late adulthood is considered to extend from the 60s on. This is the last stage of physical change. The skin continues to lose elasticity, reaction time slows further, and muscle strength diminishes. Smell, taste, hearing, and vision, so sharp in our twenties, decline significantly. The brain may also no longer function at optimal levels, leading to problems like memory loss, dementia, and Alzheimer’s disease in later years.
Link to Learning
Aging doesn’t mean a person can’t explore new pursuits, learn new skills, and continue to grow. Watch this inspiring story about Neil Unger who is a newbie to the world of skateboarding at 60 years old.
Cognitive Development
Because we spend so many years in adulthood (more than any other stage), cognitive changes are numerous. In fact, research suggests that adult cognitive development is a complex, ever changing process that may be even more active than cognitive development in infancy and early childhood (Fischer, Yan, & Stewart, 2003).
Researchers have identified areas of both losses and gains in cognition in older age. Cognitive ability and intelligence are often measured using standardized tests and validated measures. The psychometric approach has identified two categories of intelligence that show different rates of change across the life span (Schaie & Willis, 1996). Fluid intelligence refers to information processing abilities, such as logical reasoning, remembering lists, spatial ability, and reaction time. Crystallized intelligence encompasses abilities that draw upon experience and knowledge. Measures of crystallized intelligence include vocabulary tests, solving number problems, and understanding texts.

With age, systematic declines are observed on cognitive tasks requiring self-initiated, effortful processing, without the aid of supportive memory cues (Park, 2000). Older adults tend to perform poorer than young adults on memory tasks that involve recall of information, where individuals must retrieve information they learned previously without the help of a list of possible choices. For example, older adults may have more difficulty recalling facts such as names or contextual details about where or when something happened (Craik, 2000). What might explain these deficits as we age? As we age, working memory, or our ability to simultaneously store and use information, becomes less efficient (Craik & Bialystok, 2006). The ability to process information quickly also decreases with age. This slowing of processing speed may explain age differences on many different cognitive tasks (Salthouse, 2004). Some researchers have argued that inhibitory functioning, or the ability to focus on certain information while suppressing attention to less pertinent information, declines with age and may explain age differences in performance on cognitive tasks (Hasher & Zacks, 1988). Finally, it is well established that our hearing and vision decline as we age. Longitudinal research has proposed that deficits in sensory functioning explain age differences in a variety of cognitive abilities (Baltes & Lindenberger, 1997).
Fewer age differences are observed when memory cues are available, such as for recognition memory tasks, or when individuals can draw upon acquired knowledge or experience. For example, older adults often perform as well if not better than young adults on tests of word knowledge or vocabulary. With age often comes expertise, and research has pointed to areas where aging experts perform as well or better than younger individuals. For example, older typists were found to compensate for age-related declines in speed by looking farther ahead at printed text (Salthouse, 1984). Compared to younger players, older chess experts are able to focus on a smaller set of possible moves, leading to greater cognitive efficiency (Charness, 1981). Accrued knowledge of everyday tasks, such as grocery prices, can help older adults to make better decisions than young adults (Tentori, Osheron, Hasher, & May, 2001).
How do changes or maintenance of cognitive ability affect older adults’ everyday lives? Researchers have studied cognition in the context of several different everyday activities. One example is driving. Although older adults often have more years of driving experience, cognitive declines related to reaction time or attentional processes may pose limitations under certain circumstances (Park & Gutchess, 2000). Research on interpersonal problem solving suggested that older adults use more effective strategies than younger adults to navigate through social and emotional problems (Blanchard-Fields, 2007). In the context of work, researchers rarely find that older individuals perform poorer on the job (Park & Gutchess, 2000). Similar to everyday problem solving, older workers may develop more efficient strategies and rely on expertise to compensate for cognitive decline.
How can we delay the onset of cognitive decline? Mental and physical activity seems to play a part (Figure 2). Research has found adults who engage in mentally and physically stimulating activities experience less cognitive decline and have a reduced incidence of mild cognitive impairment and dementia (Hertzog, Kramer, Wilson, & Lindenberger, 2009; Larson et al., 2006; Podewils et al., 2005).
Psychosocial Development
There are many theories about the social and emotional aspects of aging. Some aspects of healthy aging include activities, social connectedness, and the role of a person’s culture. According to many theorists, including George Vaillant (2002), who studied and analyzed over 50 years of data, we need to have and continue to find meaning throughout our lives. For those in early and middle adulthood, meaning is found through work (Sterns & Huyck, 2001) and family life (Markus, Ryff, Curan, & Palmersheim, 2004). These areas relate to the tasks that Erikson referred to as intimacy versus isolation in early adulthood and generativity versus stagnation in middle adulthood. As mentioned previously, adults tend to define themselves by what they do—their careers. Earnings peak during this time, yet job satisfaction is more closely tied to work that involves contact with other people, is interesting, provides opportunities for advancement, and allows some independence (Mohr & Zoghi, 2006) than it is to salary (Iyengar, Wells, & Schwartz, 2006). How might being unemployed or being in a dead-end job challenge adult well-being?
As people enter the final stages of life, they have what Erik Erikson described as a crisis over integrity versus despair. In other words, they review the events of their lives and try to come to terms with the mark (or lack thereof) that they have made on the world. People who believe they have had a positive impact on the world through their contributions live the end of life with a sense of integrity. Those who feel they have not measured up to certain standards—either their own or others’—develop a sense of despair.

Positive relationships with significant others in our adult years have been found to contribute to a state of well-being (Ryff & Singer, 2009). Most adults in the United States identify themselves through their relationships with family—particularly with spouses, children, and parents (Markus et al., 2004). While raising children can be stressful, especially when they are young, research suggests that parents reap the rewards down the road, as adult children tend to have a positive effect on parental well-being (Umberson, Pudrovska, & Reczek, 2010). Having a stable marriage has also been found to contribute to well-being throughout adulthood (Vaillant, 2002).
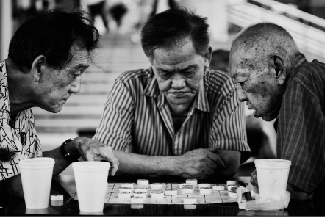
Another aspect of positive aging is believed to be social connectedness and social support. As we get older, socioemotional selectivity theory suggests that our social support and friendships dwindle in number, but remain as close, if not more close than in our earlier years (Carstensen, 1992) (Figure 3).
Link to Learning
Death and Dying
Every story has an ending. Death marks the end of your life story (Figure 1). Our culture and individual backgrounds influence how we view death. In some cultures, death is accepted as a natural part of life and is embraced. In contrast, until about 50 years ago in the United States, a doctor might not inform someone that they were dying, and the majority of deaths occurred in hospitals. In 1967 that reality began to change with Cicely Saunders, who created the first modern hospice in England. The aim of hospice is to help provide a death with dignity and pain management in a humane and comfortable environment, which is usually outside of a hospital setting. In 1974, Florence Wald founded the first hospice in the United States. Today, hospice provides care for 1.65 million Americans and their families. Because of hospice care, many terminally ill people are able to spend their last days at home.

Research has indicated that hospice care is beneficial for the patient (Brumley, Enquidanos, & Cherin, 2003; Brumley et al., 2007; Godkin, Krant, & Doster, 1984) and for the patient’s family (Rhodes, Mitchell, Miller, Connor, & Teno, 2008; Godkin et al., 1984). Hospice patients report high levels of satisfaction with hospice care because they are able to remain at home and are not completely dependent on strangers for care (Brumley et al., 2007). In addition, hospice patients tend to live longer than non-hospice patients (Connor, Pyenson, Fitch, Spence, & Iwasaki, 2007; Temel et al., 2010). Family members receive emotional support and are regularly informed of their loved one’s treatment and condition. The family member’s burden of care is also reduced (McMillan et al., 2006). Both the patient and the patient’s family members report increased family support, increased social support, and improved coping while receiving hospice services (Godkin et al., 1984).
How do you think you might react if you were diagnosed with a terminal illness like cancer? Elizabeth Kübler-Ross (1969), who worked with the founders of hospice care, described the process of an individual accepting his own death. She proposed five stages of grief: denial, anger, bargaining, depression, and acceptance. Most individuals experience these stages, but the stages may occur in different orders, depending on the individual. In addition, not all people experience all of the stages. It is also important to note that some psychologists believe that the more a dying person fights death, the more likely he is to remain stuck in the denial phase. This could make it difficult for the dying person to face death with dignity. However, other psychologists believe that not facing death until the very end is an adaptive coping mechanism for some people.
Whether due to illness or old age, not everyone facing death or the loss of a loved one experiences the negative emotions outlined in the Kübler-Ross model (Nolen-Hoeksema & Larson, 1999). For example, research suggests that people with religious or spiritual beliefs are better able to cope with death because of their hope in an afterlife and because of social support from religious or spiritual associations (Hood, Spilka, Hunsberger, & Corsuch, 1996; McIntosh, Silver, & Wortman, 1993; Paloutzian, 1996; Samarel, 1991; Wortman & Park, 2008).
A prominent example of a person creating meaning through death is Randy Pausch, who was a well-loved and respected professor at Carnegie Mellon University. Diagnosed with terminal pancreatic cancer in his mid-40s and given only 3–6 months to live, Pausch focused on living in a fulfilling way in the time he had left. Instead of becoming angry and depressed, he presented his now famous last lecture called “Really Achieving Your Childhood Dreams.” In his moving, yet humorous talk, he shares his insights on seeing the good in others, overcoming obstacles, and experiencing zero gravity, among many other things. Despite his terminal diagnosis, Pausch lived the final year of his life with joy and hope, showing us that our plans for the future still matter, even if we know that we are dying.
Link to Learning
Really Achieving Your Childhood Dreams is Randy Pausch’s last lecture. Listen to his inspiring talk.
Think It Over
- Have you ever had to cope with the loss of a loved one? If so, what concepts described in this section provide context that may help you understand your experience and process of grieving?
- If you were diagnosed with a terminal illness would you choose hospice care or a traditional death in a hospital? Why?
Licenses and Attributions (Click to expand)
CC licensed content, Original
- Provided by: Lumen Learning. License: CC BY-SA: Attribution-ShareAlike
- Modification and adaptation, addition of crash course video. Provided by: Lumen Learning. License: CC BY: Attribution
- Modification and adaptation, inclusion of tutorial. Provided by: Lumen Learning. License: CC BY: Attribution
- Signs of Aging interactive. Authored by: Jessica Traylor for Lumen Learning. Provided by: Lumen Learning. License: CC BY: Attribution
CC licensed content, Shared previously
- Socioemotional Development in Late Adulthood. Provided by: Boundless. Located at: https://www.boundless.com/psychology/textbooks/boundless-psychology-textbook/human-development-14/aging-late-adulthood-412/socioemotional-development-in-late-adulthood-292-12827/. License: CC BY-SA: Attribution-ShareAlike
- Stages of Development. Authored by: OpenStax College. Located at: https://openstax.org/books/psychology-2e/pages/9-3-stages-of-development. License: CC BY: Attribution. License Terms: Download for free at https://openstax.org/books/psychology-2e/pages/1-introduction
- Brain Changes and Cognitive Development in Adolescence. Provided by: Open Learning Initiative. Located at: https://oli.cmu.edu/jcourse/workbook/activity/page?context=df3e73250a0001dc08caae28aa5ca73a. License: CC BY-NC-SA: Attribution-NonCommercial-ShareAlike
- Section on cognitive development. Authored by: Tara Queen and Jacqui Smith . Provided by: University of Michigan. Located at: http://nobaproject.com/modules/aging. Project: The Noba Project. License: CC BY-NC-SA: Attribution-NonCommercial-ShareAlike
- Physical Development in Late Adulthood. Provided by: Boundless. Located at: https://www.boundless.com/psychology/textbooks/boundless-psychology-textbook/human-development-14/aging-late-adulthood-412/physical-development-in-late-adulthood-291-12826/. License: CC BY: Attribution
- Death and Dying. Authored by: OpenStax College. Located at: https://openstax.org/books/psychology-2e/pages/9-4-death-and-dying. License: CC BY: Attribution. License Terms: Download for free at https://openstax.org/books/psychology-2e/pages/1-introduction
All rights reserved content
- How to Be the Oldest Person Alive. Authored by: Glamour Magazine. Located at: https://www.youtube.com/watch?v=I62njq9gsaI. License: Other. License Terms: Standard YouTube License
period of development that begins at puberty and ends at early adulthood
maturing of the adrenal glands
maturing of the sex glands
organs specifically needed for reproduction
physical signs of sexual maturation that do not directly involve sex organs
beginning of menstrual period; around 12–13 years old
first male ejaculation
newly defined period of lifespan development from 18 years old to the mid-20s; young people are taking longer to complete college, get a job, get married, and start a family
information processing abilities, such as logical reasoning, remembering lists, spatial ability, and reaction time
intelligence that draw upon experience and knowledge. Measures include vocabulary tests, solving number problems, and understanding texts
service that provides a death with dignity; pain management in a humane and comfortable environment; usually outside of a hospital setting
denial, anger, bargaining, depression, and acceptance
